

Falls are one of the most persistent safety challenges across senior living and long-term care. In the United States, AHRQ estimates that about 1.3 million residents in nursing facilities fall each year. Other AHRQ nursing-facility materials state that about half of all nursing facility residents fall every year, and 30–40% of residents who fall do so at least twice. One in every ten residents who falls has a serious injury, such as a fracture, laceration, or serious head injury.
The same pressure exists across Europe. A large study of care homes in England found a fall incidence rate of 1,249 falls per 1,000 residents per year, and among residents who had already fallen, 45% had three or more falls. The study also found that residents who experienced a fall were more likely to have at least one hospitalization than residents with no documented falls.
With numbers like these, it is understandable that senior living operators look for technology that can detect falls faster. Accelerometer-based pendants, watches, belts, and wearable sensors appear to offer a simple answer: detect sudden movement, trigger an alarm, and send staff to help.
But this is where many facilities fall into the accelerometer trap. A fall is not just a spike in motion. It is a clinical, environmental, behavioral, and operational event. When senior living communities treat accelerometer alerts as a complete fall-prevention strategy, they risk solving only the easiest part of the problem: knowing that something may have happened.
Falls in senior living are not isolated incidents

A fall rarely happens in isolation. It may be connected to muscle weakness, impaired balance, poor vision, medication side effects, cognitive decline, dehydration, toileting needs, room layout, lighting, footwear, or a poorly positioned assistive device.
That complexity matters. A fall is often the visible endpoint of several risk factors that were already present before the resident reached the floor.
This is why falls affect more than immediate resident safety. They increase staff workload, family concern, documentation pressure, clinical follow-up, and sometimes emergency transfers. Even when no major injury occurs, a fall can create fear of falling, reduced mobility, loss of confidence, and further physical decline.
In memory care, the challenge is even more complex. Residents may be unable to describe the incident, identify pain location, or report if symptoms such as dizziness, confusion, toileting urgency, or environmental hazards contributed. In assisted living or life plan communities, fall risk can increase gradually as residents age and acuity rises.
Because the stakes are high, faster detection has clear value. If a resident falls and cannot call for help, the time between the event and staff awareness matters. The problem begins when detection is confused with prevention.
That distinction is where accelerometers need to be examined carefully
Why accelerometers became the easy answer to a complex problem

Accelerometers have become popular for fall detection because they are practical. They are small, relatively low-cost, easy to place in wearable devices, and capable of detecting changes in motion. A pendant, watch, or belt-worn device can monitor acceleration and trigger an alert when movement appears consistent with a fall.
On paper, the model looks clean:
- The resident wears the device.
- The device detects a rapid motion pattern.
- The system classifies the event as a fall.
- Staff receives an alert.
- The response begins faster.
For senior living communities under pressure, this promise is compelling. It suggests faster awareness, broader coverage, and less dependence on direct observation every minute.
But real-world resident movement is not clean data. Falls do not follow one standard pattern. Some residents collapse suddenly. Others slide slowly from a bed or chair. Some lose balance during transfers. Others sit down heavily, drop the device, adjust the wearable, or remove it completely.
To a motion-only system, the difference between a fall and normal movement is not always obvious. That is where the accelerometer trap begins.
What the accelerometer trap means

The accelerometer trap is the assumption that wearable motion data can solve the fall problem on its own. Accelerometers can detect sudden changes in movement, but they cannot fully explain resident intent, environmental cause, clinical risk, staff workflow, or whether an alert represents a true fall.
A fall in a senior living community is not only a kinematic event. It is a contextual event.
A sudden acceleration may mean a resident fell. It may also mean the resident sat down heavily, dropped the device, adjusted the wearable, bumped it against furniture, or moved abruptly during normal activity. At the same time, a slow slide from a bed or wheelchair may be clinically serious but may not generate the sharp acceleration pattern that a simple detection threshold expects.
From an engineering perspective, this is the core problem. The device sees a graph: signal magnitude over time. It does not see the resident’s intent, the floor, the bathroom, the chair, the walker, the caregiver response, or the clinical condition that caused the movement.
This creates a difficult trade-off. If the system threshold is too sensitive, it may create too many false alarms. If it is too strict, it may miss slower or atypical falls. Algorithms can improve classification, but they still depend on the quality and context of the signal.
Motion data is useful. But motion data alone is not equivalent to resident safety.
Accelerometer signals: why motion alone can be misleading
The following signal examples come from technical work by the Intrexis team in collaboration with Aionys engineers. They show why fall detection cannot rely only on a simple acceleration spike. The X-axis represents time, while the Y-axis represents acceleration or signal magnitude. The first two graphs represent real fall events. The third and fourth graphs show active movements that can look similar to a motion-based algorithm.
Figure 1. Real fall signal captured by accelerometer data
A real fall event can create a strong acceleration spike followed by instability in the signal. However, the shape alone does not explain the cause of the fall or the resident’s condition.
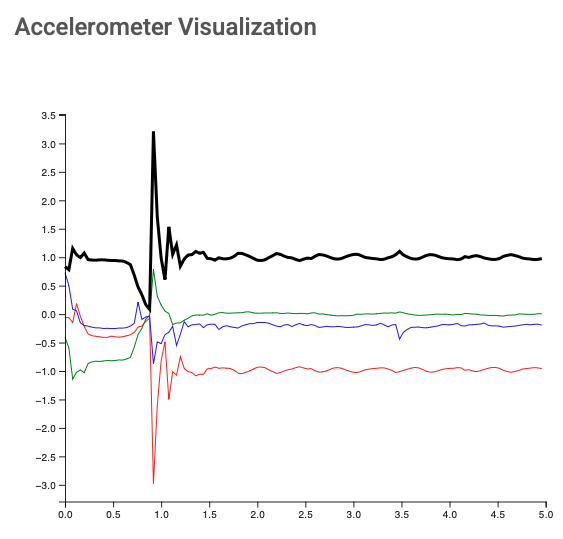
Figure 2. Real fall signal with a different acceleration pattern
Another real fall can produce a different signal profile, showing why one fixed threshold cannot reliably represent every fall scenario.
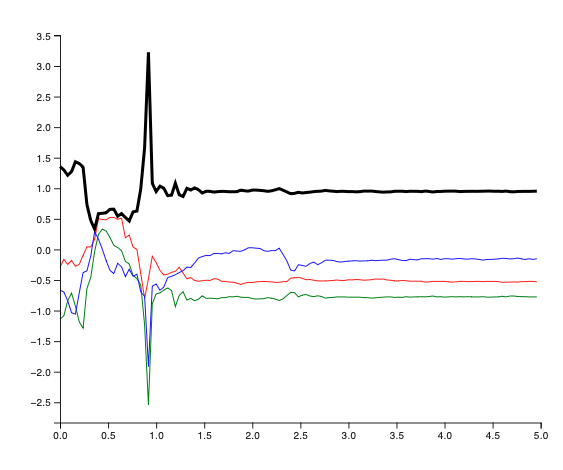
Figure 3. Active movement signal that may resemble a fall
Some non-fall movements can produce sharp signal changes, making false alerts possible when the system relies too heavily on motion alone.
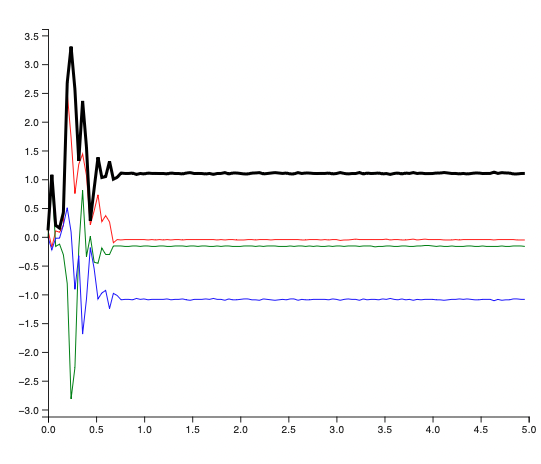
Figure 4. Active movement with a high acceleration spike
A non-fall event can sometimes generate a stronger spike than a real fall, which creates the core classification challenge for accelerometer-only detection.
Machine learning can improve this picture. Training algorithms on large volumes of real-world fall data can reduce noise and help the system recognize more patterns. But machine learning does not remove the fundamental trade-off. If the system becomes more sensitive, it may detect more real falls but also generate more false alerts.
If the system becomes stricter, false alerts may drop, but some real falls may be missed. That is why the issue is not simply whether the algorithm is advanced.
The key consideration is whether the system can provide effective fall detection without overwhelming staff or missing critical events.
The false-positive problem: when alarms become noise

False positives are not a minor technical inconvenience. In a senior living community, every alert interrupts a workflow. Someone has to stop, interpret the signal, check the resident, document the response, and then return to the original task.
Real-world studies show why this matters. In one nursing-home study, an automated fall detection device detected only 17 of 89 staff-recorded falls within an 8-hour window. Of 128 fall events recorded by the device, only 17 matched nursing reports, while 111 were false positives. The authors concluded that there was poor concordance between device-recorded falls and falls reported by nursing home staff.
Another real-world study of a wearable fall detection device in older adults recorded 84 fall alarms, of which 83 were false alarms. Many were caused by normal device use, dropping the device, putting it down, misuse, or unknown reasons.
These studies do not prove that every accelerometer-based system performs this poorly. Device design, placement, algorithms, resident population, and workflow integration all matter. But they do prove a critical point: real-world performance is different from laboratory performance.
This same issue has appeared in technical work conducted by Intrexis with Aionys' team support. In high-sensitivity configurations, accelerometer-based models may capture more fall-like events, including hard falls, but they may also generate an operationally unacceptable number of false alerts. In lower-noise configurations, false alerts can be reduced, but some real falls may be missed.
These observations should be understood as engineering insights, not universal clinical performance claims. Their value is in showing the trade-off: with accelerometer-only detection, a community often has to choose between too much noise and too much missed risk.
That is why a fall-detection tool should not be judged only by advertised accuracy or controlled testing. Senior living operators need to know what happens during ordinary shifts, with real residents, real staff constraints, real compliance issues, and real operational pressure.
The hidden cost of false fall alerts

When false alarms accumulate, the issue moves beyond technology and becomes a staff safety problem.
Alarm fatigue is a recognized healthcare phenomenon. It occurs when repeated exposure to frequent or non-actionable alarms creates sensory overload, emotional strain, desensitization, and reduced responsiveness among healthcare professionals. False alarms can significantly contribute to this problem.
Each false detection consumes staff time. It also increases cognitive load, emotional pressure, and workflow disruption. In practical terms, false fall alerts cost time, money, and attention. They pull care teams away from toileting support, direct care, medication assistance, mobility supervision, resident engagement, or another resident who may need immediate help.
For senior living communities, the risk is straightforward. If staff receive too many low-value alerts, trust in the system declines. Response may become slower. Some alert types may be mentally deprioritized. Teams may begin to treat alarms as background noise rather than actionable signals.
That outcome defeats the purpose of fall technology.
This is why ROI should not be measured only in hardware cost or detection claims. It should also include staff time, alert burden, response quality, and whether the system reduces operational pressure. A solution that protects residents while lowering unnecessary workload creates value for both care quality and community economics.
Instead of asking, "Can this device detect a fall?" nursing homes should ask: Does this system reduce harm without overwhelming the people responsible for responding?
Fall detection is not the same as fall prevention

A fall detector can tell staff that a fall may have happened. It does not, by itself, reduce the underlying reasons residents fall.
Fall prevention requires a broader view of risk. AHRQ’s Falls Management Program for nursing facilities identifies intrinsic factors such as gait, balance, strength, chronic disease, deconditioning, behavioral symptoms, and medication side effects. It also identifies extrinsic factors such as environmental hazards, unsafe equipment, poor lighting, cluttered spaces, uneven floors, wet areas, unstable furniture, ineffective wheelchair brakes, improper footwear, and inaccessible personal items.
Clinical and operational causes also matter. A resident may be at higher risk because of balance impairment, muscle weakness, confusion, medication changes, low blood pressure, visual impairment, continence needs, or unsafe transfer habits. If these factors are not addressed, a device may simply detect repeated events rather than help prevent them.
That is the limitation of motion-only thinking. It treats the fall as the starting point. In reality, the fall is often the final signal of a risk pattern that started earlier.
Prevention requires a different loop:
- Identify risk.
- Reduce hazards.
- Monitor changes.
- Respond quickly.
- Review the cause.
- Adjust the care plan.
- Prevent recurrence.
Technology becomes valuable when it strengthens this loop. It becomes dangerous when it replaces the loop.
What senior living communities should do instead

Avoiding the accelerometer trap does not mean rejecting fall-detection technology. It means placing technology inside a broader safety model.
Start with resident-level risk assessment
Fall prevention begins with knowing who is at risk and why. Communities should regularly assess fall history, mobility, cognition, medication profile, vision, continence, transfer ability, assistive device use, and environmental exposure.
A resident who falls during nighttime toileting has a different risk profile from a resident who falls during transfers or from a resident who wanders because of cognitive impairment. The prevention plan should reflect that difference.
Reduce preventable environmental hazards
Many fall risks are practical and visible: poor lighting, cluttered walkways, unstable furniture, unsafe flooring, inaccessible call points, inappropriate footwear, or assistive devices placed out of reach.
Technology cannot compensate for an unsafe physical environment. If a room layout increases transfer risk, or if a resident repeatedly falls on the way to the bathroom, the solution cannot be only another alert.
Design staff response workflows before adding alarms
An alarm is only useful if the response is clear.
Before deploying any fall-detection system, senior living communities should define who receives alerts, how escalation works, which alerts require immediate checks, how staff confirm a false alarm, and how events are documented.
Without workflow design, technology creates more signals but not necessarily better action.
Track alarm quality, not just alarm volume
Communities should measure true positives, false positives, missed events, response time, repeated fall locations, resident compliance, and staff feedback. If an alert system increases workload without improving response or prevention, it needs recalibration.
The goal is not more alarms. The goal is better decisions.
Review every serious fall for root cause
A post-fall review should not stop at documentation. It should ask what happened before the fall, what the resident was trying to do, what environmental factors were present, whether medications or clinical status changed, and what intervention could reduce recurrence.
This is where simple accelerometer data is often weakest. It may confirm that motion occurred, but it may not explain why the resident fell.
Conclusion: Detection Is Not Prevention

Accelerometers can be useful. They can help detect certain types of falls and support faster notification when the signal is accurate, the resident wears the device, and the workflow is well designed.
But accelerometers are not a complete fall-prevention strategy.
Senior living communities fall into the accelerometer trap when they confuse motion detection with resident safety. A fall is not only a movement pattern. It is the result of clinical risk, environmental conditions, resident behavior, staff workflow, and response design.
The real goal is not simply to know that motion occurred. The real goal is to reduce harm.
That requires fewer false alarms, faster response, better context, stronger workflows, and a prevention model that learns from every event.
Senior living operators should not ask only whether a device can detect a fall. They should ask whether the entire system helps prevent the next one.